By Grace Nthemba, December, 2025.
In a world obsessed with standing straight and fitting in, those living with scoliosis are flipping the script, proving that confidence has nothing to do with the angle of your spine and everything to do with how you carry yourself.
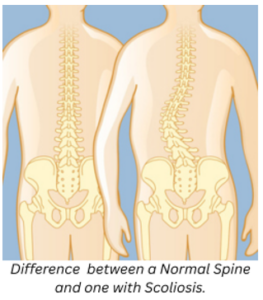
Scoliosis is a condition whereby the spine curves abnormally to the side. The curve often resembles either a ‘C’ shape or an ‘S’ shape as opposed to being straight.
Not all scoliosis is created equal. Doctors classify the condition into several categories based on its cause and timing. Idiopathic scoliosis accounts for about 80% of cases. “Idiopathic” is medical terminology for “we don’t know why it happens,” though researchers suspect genetic factors play a role. This type is further divided by age: infantile (0-3 years), juvenile (4-10 years), and adolescent (11-18 years), with adolescent idiopathic scoliosis being by far the most common. Congenital scoliosis is present at birth, resulting from vertebrae that didn’t form properly during fetal development. This rarer form may be detected in infancy or early childhood and sometimes requires earlier intervention.
Neuromuscular scoliosis develops as a secondary condition in people with neurological or muscular disorders such as cerebral palsy, muscular dystrophy, or spina bifida. These curves tend to progress more rapidly and often require different treatment approaches.
Degenerative scoliosis affects adults, typically those over 65, as the spine’s discs and joints wear down with age. This “adult-onset” scoliosis can cause significant pain and differs markedly from the curves that develop during childhood.
According to the Spine Correction Center, research shows that girls are significantly more likely to experience curve progression that boys during the adolescent window, as this is when they experience a growth spurt. The symptoms which are presented may include; one shoulder being higher than the other or one hip being more prominent than the other.
Treatment for scoliosis isn’t one-size-fits-all. It depends on the curve’s severity, the patient’s age, and whether the spine is still growing. Bracing becomes the standard recommendation for moderate curves (25-40 degrees) in children who are still growing. Modern braces are far less cumbersome than their predecessors, and many can be worn under clothing. The brace doesn’t reverse the curve but can prevent it from worsening during growth. Sarah wore a Boston brace for eighteen hours daily through her teenage years—a challenging experience she describes as “annoying but manageable once I got used to it.”
Surgery is typically reserved for curves exceeding 45-50 degrees or curves that continue progressing despite bracing. Spinal fusion, the most common surgical procedure, involves fusing together curved vertebrae using bone grafts and metal rods to straighten the spine. While this limits flexibility in the fused area, most patients adapt well and experience significant improvements in appearance and, when present, pain relief.
Research continues to unlock scoliosis’s mysteries. Scientists are investigating genetic markers that might predict which curves will progress, potentially allowing for earlier, more targeted interventions. New bracing technologies are becoming more comfortable and effective. Surgical techniques grow increasingly refined, with some procedures now performed using minimally invasive approaches.
Perhaps most importantly, awareness is growing. School screening programs catch curves early when treatment is most effective. Medical professionals better understand the psychological impact of diagnosis and treatment, especially on adolescents navigating an already challenging time of life.
Scoliosis may cause the spine to take a different path, but it doesn’t prevent people from reaching their destinations. With proper monitoring, appropriate treatment when needed, and support from medical professionals and loved ones, those with scoliosis can thrive—curves and all.